Dentistry >>>> Why can't a removable denture hold?
Why can't a removable denture hold?

When a person is faced with the fact of complete loss of teeth and the need for prosthetics with full dentures, the problem of retention of such prostheses in the oral cavity often comes to the surface, since not all forms of the alveolar processes of the jaw are suitable for perfect retention of full dentures.
How is a removable denture hold? The denture on the edentulous jaw is retained due to several factors. To begin with, it must adhere to the surface of the mucous membrane lining the jaw due to the phenomenon of adhesion (according to the principle of a rubber suction cup), that is, when saliva, the movable mucous membrane and the hard inner surface of the prosthesis form a single whole for a while.
When a person begins to chew food with prostheses, the prosthesis on the edentulous jaw is held and does not move due to the convex shape of the ridge of the alveolar ridge of the jaw and various anatomical features of the surface of the prosthetic jaw bed, which are able to hold the prosthesis during chewing - preventing it from moving from the prosthetic bed and thereby preventing separation of the "stuck" prosthesis and the mucosal surface.
Such special retaining elements on the jaw are bony protrusions (well placed and not traumatized when the prosthesis is worn), undercuts (depressions) in the lower jaw (sublingual regions in the lateral parts of the alveolar process of the lower jaw), a slightly overhanging ridge of the alveolar process (and not sloping, with which the prosthesis will "slide down" like a skier from a hill), moderately convex tubercles of the right and lower jaw, and of course the rather high alveolar process of the jaw itself.
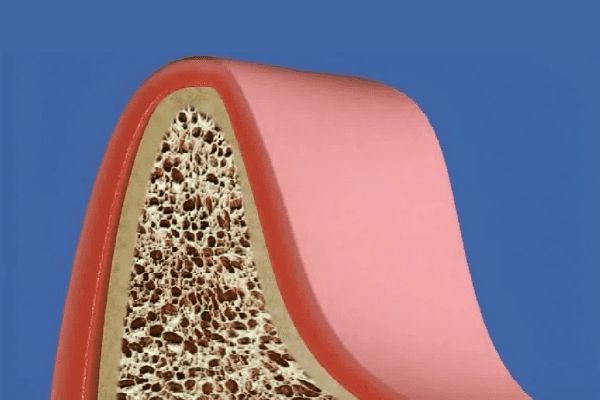
A set of successful anatomical structures on the jaw is a guarantee of a fully removable denture that fits well when talking and chewing food. But often all possible successful anatomical features of the jaw in the period after the complete loss of teeth are useless due to the complete atrophy of the alveolar process (smoothing of the volumetric contours). In many cases, even Korega fixing gel does not help.
Why can't a removable denture hold? A removable denture is not held on the jaw when there are no physiological or anatomical conditions for holding it. Two things can interfere with the retention of a removable denture on the jaw when talking or eating:
- There is nothing to hold on to - the alveolar process of the jaw is completely atrophied.
- There is something to hold on to, but the movable strands of the cheeks and lips are located in such a way that when the jaw moves, they begin to stretch, move and throw off (displace) the denture from the prosthetic bed.
Removable denture does not hold - what to do?
Today, orthopedic dentistry and maxillofacial surgery offer several solutions to this problem:
Under good anatomical conditions to hold the full-removable prosthesis, but with movable cords of the mucous membrane, the latter are incised, which leads to the stabilization of the full-removable prosthesis on the jaw.
In the absence of favorable anatomical conditions for holding the removable denture on the jaw:
It is possible to artificially create anatomical retaining elements of the bone tissue on the prosthetic bed by provoking the growth of bone tissue in the places needed for prosthetics with the help of osteotropic drugs. Such osteotropic substances initiate the processes of growth (proliferation) of bone tissue according to a given plan of reconstruction of the prosthetic jaw bed, and after finishing their "work", they dissolve by themselves. Osteotropic substances are implanted into the bone tissue, closed with a special collagen membrane (protection against premature resorption) and begin the process of bone tissue regeneration in the required volume.

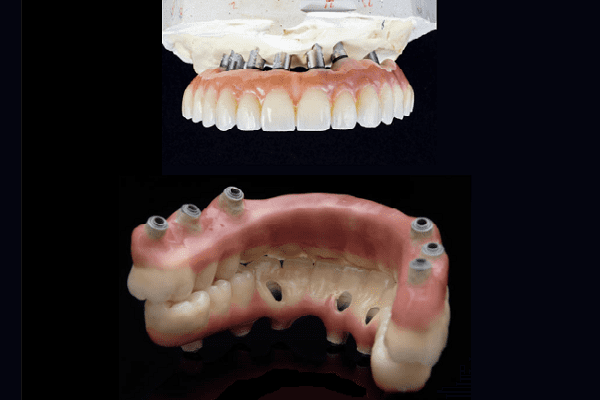
To implant the implants into the cortical bone of the jaw, since all the overlying layers of the jaw bone tissue can be destroyed by resorption (this is the cause of bone tissue atrophy) - the procedure is called "basal implantation". On several deeply implanted implants (2-4-6 and more, if necessary), serving for support, a full plate prosthesis will be planted, which will automatically turn from a removable structure into a non-removable one.
Anatomically restore the ridge of the alveolar process of the jaw using bone grafting - increasing its volume due to a natural bone graft (usually taken from the chin bone) or artificial implant materials (based on calcium phosphates, ceramics, biocomposites), and after This is to carry out prosthetics with complete removable dentures in the usual way.
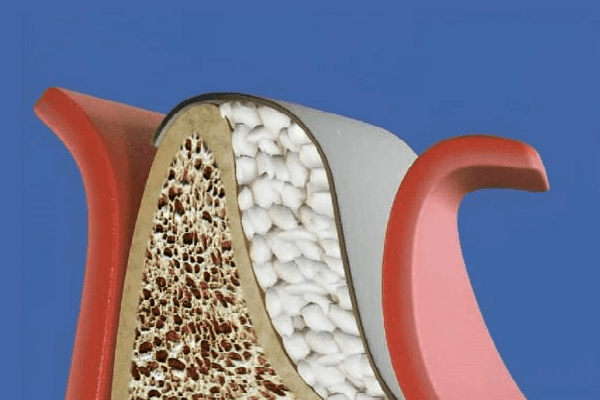
Splitting of the alveolar process followed by the introduction into the cleft of the biocomposite material Osteomatrix (crumb or monoblock) - a biological substance that imitates the structure of bone tissue and is biologically capable of reconnecting with the surrounding bone tissue. The operation is called "splitting the alveolar bone". Such an operation is aimed at thickening the alveolar process of the jaw, at increasing the height of the alveolar process, or at the segmented creation of anatomical protrusions in the area of the alveolar process of the jaw.
Apply a combined method, including the simultaneous restoration of areas of bone tissue of the alveolar process followed by implantation of the implant - the procedure is called "sinus lifting".
The decision on the choice of the most successful method of restoring the shape and height of the alveolar process for subsequent prosthetics and methods of fixing the future removable denture is made by the doctor, correlating it with the current conditions and the state of the jaw bone tissue, and also taking into account the patient's general health and the history of the disease, which should not interfere with the course of regenerative processes in the oral cavity and bone structures of the jaw.









Read
Read